Tumours can be destroyed in many ways. Radiotherapy uses beams of ionizing radiation to damage DNA and destroy tumour cells. A less common approach is photodynamic therapy, which uses a light-activated drug to kill cancer cells via mitochondrial damage. Then there’s the emerging technique of radiodynamic therapy (RDT).
“Radiodynamic therapy is the combination of radiotherapy plus photodynamic therapy,” explained Charlie Ma from Fox Chase Cancer Center, speaking at the recent AAPM Annual Meeting.
Photodynamic therapy typically uses visible laser light to activate a photosensitive drug that’s preferentially localized within tumour cells. The activated drug generates highly cytotoxic singlet oxygen that causes cell death. The limited penetration of laser light into tissue, however, means that the technique is mainly used to treat superficial tumours or sites with endoscopic access. To treat deep-seated tumours that photodynamic therapy cannot reach, RDT uses high-energy photon beams to activate the photosensitizer.
“In RDT, we use 20 to 30 per cent of the dose from radiotherapy,” Ma explained. “And then we also use the Cherenkov light.” He noted that this Cherenkov radiation, which is generated during radiotherapy as the treatment beam interacts with the patient’s tissue, will have an almost identical light distribution to the therapeutic radiation dose distribution and thus can be easily planned.
In addition to accumulating in the primary tumour, the drug will also be absorbed by distributed metastatic cells, which can be killed using a very low dose of Cherenkov light. “Now for the first time, RDT makes radiotherapy not only local and regional, but a systemic treatment technique,” said Ma.
The team at Fox Chase is using a drug called 5-aminolevulinic acid (5-ALA) for RDT. 5-ALA is taken up by the mitochondria in cancer cells, with 10 to 20 times greater uptake in tumours than in normal tissues. Once inside a cancer cell, 5-ALA is metabolized into protoporphyrin IX (PpIX), a photosensitizer with an absorption spectrum peak at around 380–430 nm. This is not ideal for the red laser light often used for photodynamic therapy. It is, however, a great match for the Cherenkov absorption peak at 370–430 nm.
Preclinical proof
Over the last few years, Ma and his team have performed many preclinical studies using different tumour cell lines and various radiation energies. He shared some results from a large study (several hundred animals) assessing RDT of tumour-bearing mice using 100 mg/kg 5-ALA and 6, 15 or 45 MV photon irradiation.
Ma noted that the tumour was highly aggressive, with 4 Gy of radiotherapy alone only killing about 10% of the tumour cells. In addition, RDT at 6 MV did not significantly increase the therapeutic effect. “That’s why people worried that Cherenkov light is not sufficient,” he noted. “But with 15 and 45 MV you see far more tumour growth delay. We are still studying why there is this dramatic change due to energy, we need to find the exact mechanism behind it.”
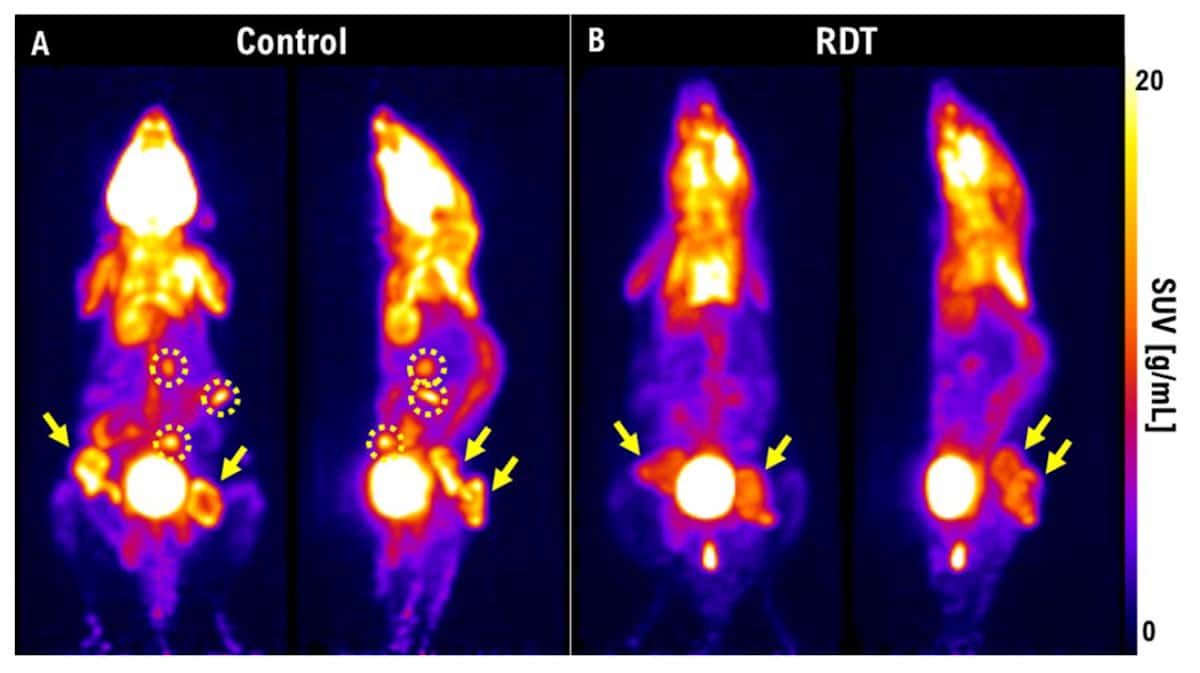
The team used PET to visualize tumour shrinkage after RDT. One week post-treatment, tumours in control mice had grown and metastasized, while those treated with RDT had much smaller lesions and no metastases. Ma also described a study of a highly aggressive thyroid cancer in rabbits. One week after 3 Gy of radiotherapy, the tumour was still growing. “But if we use RDT at 3 Gy with 5-ALA, the tumour was not seen on the PET images.” He emphasized that PET provides an excellent way to perform early treatment evaluation and could help determine whether or not RDT would be effective in a patient.
Fox Chase is now performing a clinical trial on RDT, with the first phase of the study examining dose escalation (both radiation dose and drug dose) in late-stage tumours. This phase has now reached the final dose level with just three patients left, said Ma, pointing out that so far no toxicities had occurred in any cases. Elsewhere, a second RDT trial at University Hospital Muenster is examining patients with a first recurrence of glioblastoma.
Real-life cases
Finally, Ma presented results from a number of real-life cases. “You will be excited to see these,” he told the audience, noting that “usually, people don’t believe it works unless you have one month imaging with CT, MR or PET”.
In the first example, a treatment of liver metastases, he showed that one month after RDT, PET imaging revealed that no tumours remained. Next, he presented a case of lung cancer with metastases: “you can see very dramatic results with tumours deactivated after RDT,” he said.

Implantable device delivers personalized photodynamic therapy
Other successful RDT treatments included an oesophageal cancer, a lung tumour with multiple bone metastases, and a patient that had failed chemotherapy but had a good response three days following RDT. Ma noted that most of the patients had late-stage cancers and had failed other treatments. “We do see an effect, so hopefully we can improve their survival,” he added.
“RDT can be a local, regional and systemic treatment that combines radiotherapy and photodynamic therapy,” Ma concluded. “We have a lot of in vitro and in vivo experiments to demonstrate its therapeutic potential, and although clinical trials are few, I hope we will have more results in the future and make this into something really useful.”
- SEO Powered Content & PR Distribution. Get Amplified Today.
- PlatoData.Network Vertical Generative Ai. Empower Yourself. Access Here.
- PlatoAiStream. Web3 Intelligence. Knowledge Amplified. Access Here.
- PlatoESG. Automotive / EVs, Carbon, CleanTech, Energy, Environment, Solar, Waste Management. Access Here.
- BlockOffsets. Modernizing Environmental Offset Ownership. Access Here.
- Source: https://physicsworld.com/a/radiodynamic-therapy-harnessing-light-to-improve-cancer-treatments/